Partial Achilles Tendon Rupture Surgery Cost
Overview
 The Achilles tendon is the extension from the two large muscles in the calf region, the gastrocnemius and the soleus. These two muscles combine to form the Achilles tendon. The tendon forms in the lower one third of the leg and extends to the back of the heel bone (calcaneus). When the muscles of the calf contract this produces tension on the Achilles tendon pulling on the back of heel causing the heel to rise and the foot to point downward. It is during this motion that high-tension force is transmitted through the Achilles tendon during pushing and jumping activity. This high tension force can cause the Achilles tendon to tear or rupture. This happens in 3 common locations. The most common location for a tendon tear is within the tendon substance just above the heel. The second and third most common locations are where the Achilles tendon attaches into the heel bone and higher in the leg, where the tendon begins.
The Achilles tendon is the extension from the two large muscles in the calf region, the gastrocnemius and the soleus. These two muscles combine to form the Achilles tendon. The tendon forms in the lower one third of the leg and extends to the back of the heel bone (calcaneus). When the muscles of the calf contract this produces tension on the Achilles tendon pulling on the back of heel causing the heel to rise and the foot to point downward. It is during this motion that high-tension force is transmitted through the Achilles tendon during pushing and jumping activity. This high tension force can cause the Achilles tendon to tear or rupture. This happens in 3 common locations. The most common location for a tendon tear is within the tendon substance just above the heel. The second and third most common locations are where the Achilles tendon attaches into the heel bone and higher in the leg, where the tendon begins.
Causes
A rupture occurs when a patient overstretches the Achilles tendon, an act which causes it to tear partially or completely. Achilles tendon ruptures can occur during athletic play or any time the tendon is stretched in an unexpected way.
Symptoms
Typically patients present with sudden onset of pain and swelling in the achilles region, often accompanied by a audible snap during forceful dorsiflexion of the foot. A classic example is that of an unfit 'weekend warrior' playing squash. If complete a defect may be felt and the patient will have only minimal plantar flexion against resistance.
Diagnosis
A doctor will look at the type of physical activity you have been doing. He or she will then look at your foot, ankle and leg. An MRI may also be used. This is to help determine the severity of the tear and the extent of separation of the fibers.
Non Surgical Treatment
A physical therapist teaches you exercises to help improve movement and strength, and to decrease pain. Use support devices as directed. You may need crutches or a cane for support when you walk. These devices help decrease stress and pressure on your tendon. Your caregiver will tell you how much weight you can put on your leg. Ask for more information about how to use crutches or a cane correctly. Start activity as directed. Your caregiver will tell you when it is okay to walk and play sports. You may not be able to play sports for 6 months or longer. Ask when you can go back to work or school. Do not drive until your caregiver says it is okay. 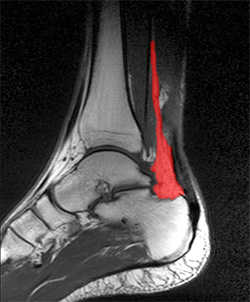
Surgical Treatment
In general, for complete tear of the tendon, surgery is recommended. For partial tears, nonsurgical treatment is recommended. However, the selection of treatment depends on the patient, age, level of activity, and other risk factors. Surgery for Achilles tendon rupture is now routine and well established. Surgery is generally suggested for the young, healthy and active individuals. For athletes, surgery is often the first choice of treatment. The Achilles tendon can be repaired surgically by either a closed or open technique. With the open technique, an incision is made to allow for better visualization and approximation of the tendon. With the closed technique, the surgeon makes several small skin incisions through which the tendon is repaired. Irrespective of type of treatment, a short leg cast (plaster) is applied on the operated ankle after completion of the procedure. The advantages of a surgical approach includes a decreased risk of re-rupture rate (0%-5%) the majority of individuals can return to their original sporting activities (within a short time), and most regain their strength and endurance. Disadvantages of a surgical approach include hospital admission, wound complications (for example, skin sloughing, infection, sinus tract formation, sural nerve injury), higher costs, and hospital admission.
Acquired Flat Foot Tibialis Posterior Tenosynovitis
Overview
A variety of foot problems can lead to adult acquired flatfoot deformity (AAFD), a condition that results in a fallen arch with the foot pointed outward. Most people - no matter what the cause of their flatfoot - can be helped with orthotics and braces. In patients who have tried orthotics and braces without any relief, surgery can be a very effective way to help with the pain and deformity. This article provides a brief overview of the problems that can result in AAFD. Further details regarding the most common conditions that cause an acquired flatfoot and their treatment options are provided in separate articles. Links to those articles are provided. 
Causes
Flat footedness, most people who develop the condition already have flat feet. With overuse or continuous loading, a change occurs where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Inadequate support from footwear may occasionally be a contributing factor. Trauma or injury, occasionally this condition may be due to fracture, sprain or direct blow to the tendon. Age, the risk of developing Posterior Tibial Tendon Dysfunction increases with age and research has suggested that middle aged women are more commonly affected. Other possible contributing factors - being overweight and inflammatory arthritis.
Symptoms
The types of symptoms that may indicate Adult-Acquired Flat Foot Deformity include foot pain that worsens over time, loss of the arch, abnormal shoe wear (excessive wearing on the inner side of shoe from walking on the inner side of the foot) and an awkward appearance of the foot and ankle (when viewed from behind, heel and toes appear to go out to the side). It is important that we help individuals recognize the early symptoms of this condition, as there are many treatment options, depending upon the severity, the age of the patient, and the desired activity levels.
Diagnosis
Looking at the patient when they stand will usually demonstrate a flatfoot deformity (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side. This leads to the presence of a ?too many toes? sign. This sign is present when the toes can be seen from directly behind the patient. The gait is often somewhat flatfooted as the patient has the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot. The physician?s touch will often demonstrate tenderness and sometimes swelling over the inside of the ankle just below the bony prominence (the medial malleolus). There may also be pain in the outside aspect of the ankle. This pain originates from impingement or compression of two tendons between the outside ankle bone (fibula) and the heel bone (calcaneus) when the patient is standing.
Non surgical Treatment
Nonoperative treatment of stage 1 and 2 acquired adult flatfoot deformity can be successful. General components of the treatment include the use of comfort shoes. Activity modification to avoid exacerbating activities. Weight loss if indicated. Specific components of treatment that over time can lead to marked improvement in symptoms include a high repetition, low resistance strengthening program. Appropriate bracing or a medial longitudinal arch support. If the posterior tibial tendon is intact, a series of exercises aimed at strengthening the elongated and dysfunctional tendon complex can be successful. In stage 2 deformities, this is combined with an ankle brace for a period of 2-3 months until the symptoms resolve. At this point, the patient is transitioned to an orthotic insert which may help to support the arch. In patients with stage 1 deformity it may be possible to use an arch support immediately. 
Surgical Treatment
In cases of PTTD that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Symptomatic flexible flatfoot conditions are common entities in both the adolescent and adult populations. Ligamentous laxity and equinus play a significant role in most adolescent deformities. Posterior tibial tendon dysfunction (PTTD) is the most common cause of adult acquired flatfoot. One should consider surgical treatment for patients who have failed nonoperative therapy and have advancing symptoms and deformities that significantly interfere with the functional demands of daily life. Isolated Joint Fusion. This technique is used for well reducible flat foot by limiting motion at one or two joints that are usually arthritic. The Evans Anterior Calcaneal Osteotomy. This is indicated for late stage II adult acquired flatfoot and the flexible adolescent flatfoot. This procedure will address midtarsal instability, restore the medial longitudinal arch and reduce mild hind foot valgus. The Posterior Calcaneal Displacement Osteotomy (PCDO). This technique is indicated for late stage I and early stage II PTTD with reducible Calcaneal valgus. This is often combined with a tendon transfer. A PCDO is also indicated as an adjunctive procedure in the surgical reconstruction of the severe flexible adolescent flatfoot. Soft tissue procedure. On their own these are not very effective but in conjunction with an osseous procedure, soft tissue procedures can produce good outcome. Common ones are tendon and capsular repair, tendon lengthening and transfer procedures. Flat foot correction requires lengthy post operative period and a lot of patience. Your foot may need surgery but you might simply not have the time or endurance to go through the rehab phase of this type of surgery. We will discuss these and type of procedures necessary for your surgery in length before we go further with any type of intervention.